¨A 32-year-old woman presented to the emergency department with a 3-day history of epigastric pain, vomiting, increasing pallor, and dark urine. Her medical history disclosed no abnormal findings. Physical examination revealed mild jaundice, abdominal distention, and bilateral lower extremity edema. Laboratory studies disclosed anemia, with a hemoglobin level of 70 g/L (7.0 g/dL), where the normal range is 115–160 g/L (11.5–16.0 g/dL). Hyperbilirubinemia was also disclosed, with a total serum bilirubin level of 75.2 μmol/L (4.4 mg/dL), where the normal range is 0–17.1 μmol/L (0–1.0 mg/dL). Liver enzyme levels were elevated, with an alanine aminotransferase, or ALT, level of 51 U/L (normal range, 5–37 U/L) and an aspartate aminotransferase, or AST, level of 170 U/L (normal range, 10–37 U/L). Serum creatinine level was normal. Findings at abdominal radiography showed a small amount of bowel gas but disclosed no other abnormalities. Abdominal ultrasonography (US) , contrast material–enhanced computed tomography (CT) , and contrast-enhanced magnetic resonance (MR) imaging were performed, in that order.¨
IMAGING FINDINGS
US depicted an echogenic thrombus in the intrahepatic inferior vena cava, a prominent caudate lobe, and mild diffuse heterogeneity of the liver parenchyma. Contrast-enhanced CT depicted a filling defect in the inferior vena cava that extended into the left hepatic vein, preferential enhancement of the central liver and an enlarged caudate lobe, mild ascites, and a filling defect in the portal vein. Findings at contrast-enhanced MR imaging confirmed the filling defects in the inferior vena cava and portal vein and also showed a diffuse reduction in renal cortical signal intensity.
Marchiafava-Micheli syndrome
It is corpuscular ADQUIRED hemolytic anemia due to the mutation of gen PIG-A in hematopoietic cells . All of hemolytic anemia are congenital except this type of corpuscular anemia. All of our cells have two molecules in the membrane called CD55 and CD59. They protect us from the action of the complement which produces their lysis. If we don´t have these molecules, the complement lysis of cells and we will have hemolytic anemia, leucopenia and trombopenia (PANCITOPENIA) and red urine. But be careful, although we see trombopenia , patiens suffer trombosis in rare localizations like suprahepatic veins (Budd- Chiari Syndrome) and that´s the reason why this patients could die.

DIAGNOSIS
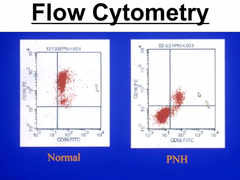
Flow cytometry (we will not see CD 55 or CD59).
Ham test: The test involves placing red blood cells in mild acid. The acid induces the activation of the complement and lysis of red blood cells.
Sucrose test: induces too the activation of the complement and hemolysis.
TREATMENT
1) Steroids
2) Anticoagulation
3) Blood transfusion
4) Fe
5) ECULIZUMAB: anti C5 complement

6) Hematopoietic stem cell transplantation: curative treatment
http://radiology.rsna.org/content/225/1/67.full